-Appendicitis is the most common cause of surgical abdomen in the pediatric age group
-presents as periumbilical diffuse abdominal pain localizing to the right lower quadrant with nausea and vomiting and fever
-The diagnosis is made clinically, labs are of limited value. WBC may be moldy elevated. Pyuria and ketonuria are limited diagnostic help
-Physical exam reveals tenderness at McBurney's point.
-Psoas- maneuver involving flexing the leg against resistance to exacerbate retro-cecal appendix
-Obturator - maneuver involving abducting the hip and flexing hip to exacerbate retro-cecal appendix
-CT scans of abdomen and Pelvis or ultrasound can be used to diagnose appendicitis
-Perforation is more likely to occur in children because the flimsy omentum and delay the diagnosis
-If the diagnosis is in question, and clinical picture is consistent with appendicitis, the patient should be observed
-
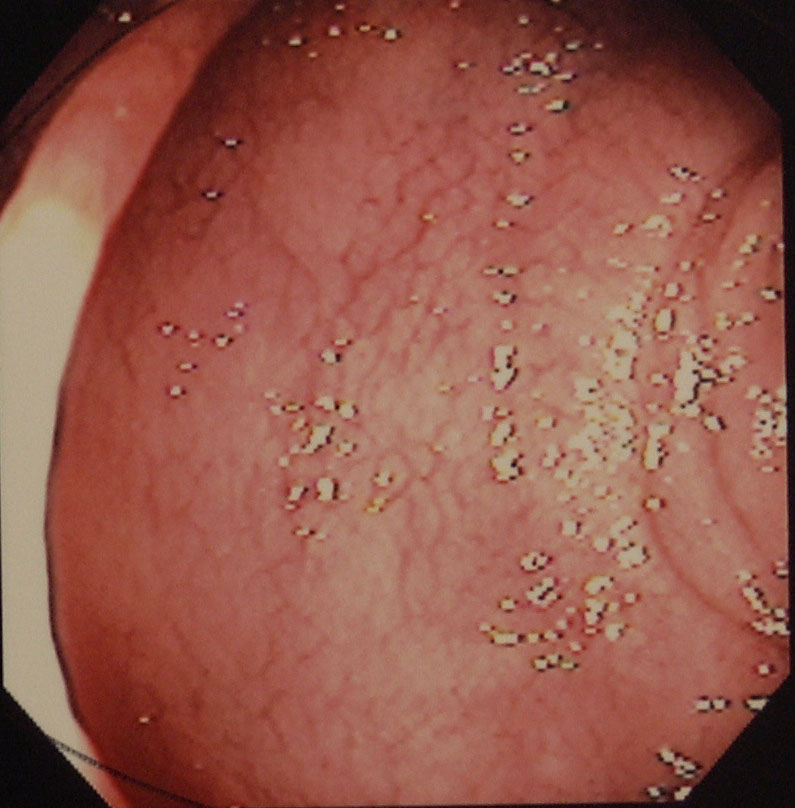
Celiac Disease-
-Celiac disease is characterized by mucosal inflammation, villous atrophy, and crypt hyperplasia that occurs with exposure to gluten diets and improve when gluten is improved
-Testing for celiac disease should be considered for those with clinical manifestations that may be representative of celiac disease
-Clinical manifestations of celiac disease include: recurrent diarrhea, malabsorption, weight loss, abdominal dissension, bloating, iron deficiency anemia, folate deficiency, vitamin B12 deficiency, persistent elevation of serum transaminases, short stature, delayed puberty, recurrent fetal loss, low birth weight infants, infertility, aphthous stomatitis, dental enamel hypoplasia, idiopathic peripheral neuropathy, cerebellar ataxia, recurrent migraine headaches, first degree relatives with diagnosis, and those with Down's Syndrome
-Immunoglobulin A (IgA) anti-tissue transglutaminase (TTG) antibody is the single preferred test for detection of celiac disease in individuals over the age of two years
-When there is a high likelihood of celiac disease the total IgA should be measured
-Can also measure both IgA and IgG based testing such as IgG deaminated gliadin peptides (DGP's) in patients with a high probability of celiac disease.
-In patients that have low IgA or IgA deficiency is identified, IgG based testing (IgG DGP's and IgG TTG) should be performed
-Patients with positive serology should undergo a small bowel biopsy to confirm the diagnosis of celiac disease
-There are many non gastrointestinal manifestations of celiac disease and they include: headache, peripheral neuropathy, ataxia, depression, anxiety, epilepsy, arthritis, iron deficiency, metabolic bone disease, hyposplenism, kidney disease, and idiopathic pulmonary hemosiderosis
-Mainstay of treatment is going on a gluten free diet
-
Constipation-
-Constipation is defined as stool frequency of less than three times per week
-Secondary causes of constipation include: obstructing lesions of the GI tract, diabetes mellitus, hypothyroidism, anorexia nervosa.
-Hirschsprung disease and functional outlet disorder can lead to impairment of defecation
-Megacolon and megarectum patients snake a small percentage with constipation
-Lab evaluation, endoscopic evaluation, and radiologic studies should be performed on selected individuals with chronic constipation and failure response to traditional therapy.
-After evaluation for structural problems, metabolic evaluation, and baseline labs, there should be a trial of fiber and laxatives
-if there is a failure of this therapy, there should be anorectal manometry and a balloon expulsion test
-Bulk forming laxatives include Metamucil, Citrucel, Fiber Con, and Benefiber
-Surfactants such as Colace are intended to lower the surface tension of stool
-Osmotic agents such as GoLytely, Lactulose, and Magnesium Citrate cause intestinal water secretion and thereby increases stool frequency
-Stimulant laxatives such as dulcolax and senna primarily exert their effects by alteration of electrolyte transport by intestinal mucosa
-
Diverticular Disease-
-Diverticulum is a sac like protrusion from the colonic wall
-Diverticulosis is the presence of diverticula
-Diverticular disease is clinically significant and symptomatic diverticulosis due to diverticular bleeding, diverticulitis, segmental colitis, associated with diverticula, or symptomatic uncomplicated diverticular disease
-Diverticular bleeding is painless hematochezia due to weakness of the vasa recta associated with diverticulum
-Diverticulitis is defined as inflammation of the diverticulum. Can be complicated by abscess, fistula, bowel obstruction, or free perforation
-Studies have shown low dietary fiber predisposes to the development of diverticular disease
-Studies have also shown an increase in diverticular disease high fat and red meat
-Seeds and its are not associated with an increase in risk for diverticulosis, diverticulitis, or diverticular bleeding
-Obesity and smoking has been associated with an increase in risk of both diverticulitis and diverticular bleeding
-Diverticula develop at well defined points of weakness, which correspond to where the vasa recta penetrate through the circular muscle layer of the colon
-Uncomplicated diverticulitis is diverticulitis without inflammatory complications such as perforation or abscess. Up to 30 percent will require surgical intervention
-Complicated diverticulitis refers to the presence of perforation, obstruction, abscess, or fistula. Nearly all these patents will require surgery
-Usual outpatient management includes Cipro 500 mg BID plus Flagyl 500 mg TID or Augmentin BID for 10-14 days
-For patients that are intolerant to flagyl, Clindamycin is acceptable alternative
-Outpatient diet recommendations are for a clear liquid diet
-Patients with complicated diverticulitis should be treated with IV antibiotics for gram negative and anaerobic pathogens
-Recommended IV antibiotics for complicated diverticulitis include Unaysn or Zosyn/ or Rocephin plus Flagyl
-Complications of diverticulitis include: peritonitis, obstruction, abscess, perforation, and fistulas
-Indications for operative management include: sepsis, diffuse peritonitis, treat a fistula, or abscess
-Goals of surgery include to remove septic focus by resection, to treat a fistula, and to restore the bowel continuity
-Resection of the diverticulosis is considered curative for diverticulosis
-
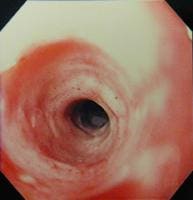
Inflammatory Bowel Disease (IBD)-
-Inflammatory Bowel Disease refers to primarily ulcerative colitis (UC) and Crohn's disease
-Ulcerative colitis is an inflammatory disorder limited to the colon
-Etiology of UC is unknown
-UC involves inflammation of the mucosal surface, and is not transmural
-UC always begins at the rectum
-UC presents with blood diarrhea, abdominal cramping, and stools often have mucus with the blood
-UC may also present with anorexia and weight loss
-Toxic megacolon is a rare complication of UC
-Patients with UC present with diarrhea and maybe blood or mucus, colicky abdominal pain, urgency, tenesmus, and incontinence. May have some weight loss. These symptoms are usually gradual and presents over several weeks.
-Extracolonic manifestations of UC include peripheral arthritis, erythema nodosum, scleritis, iritis, conjunctivitis, primary sclerosing cholangitis, venous and arterial embolism, airway inflammation, and aphthous ulcers
-Can get strictures as a complication of UC
-Mild UC management includes sulfasalazine and systemic steroids
-More severe UC should be admitted with NG decompression, ACTH if not on steroids, high dose parenteral steroids, H2 blockers and IV fluids
-Cyclosporin and Infliximab can induce remission in patients with fulminant UC
-Colectomy is curative for patients with UC and is an option for those who fail medical treatment
-Crohn's Disease (CD) is characterized by transmural inflammation of the GI tract.
-CD can occur anywhere from the mouth to the anus
-Most common part of alimentary canal affected is the terminal ileum
-Clinical symptoms of CD are: fatigue, diarrhea, abdominal pain, weight loss, fever, may have diarrhea with or without bleeding
-Complications of CD include phlegmon and abscess, perineal disease such as fissures, malabsorption, aphthous ulcers, odynophagia, dysphagia, gallstones
-Manifestations outside of the GI tract include: arthritis, uveitis, iritis, episcleritis, erythema nodosum, primary sclerosing cholangitis, secondary amyloidosis, venous and arterial embolism, renal stones, bone loss and osteoporosis, Vitamin B12 deficiency, and pulmonary development
-diagnosis of CD and UC are definitively made of tissue biopsy during endoscopy
-Treatment of CD includes sulfasalazine, mesalamine, glucocorticoids, immunomodulators (azathioprine, methotrexate), and biologic therapies (infliximab, and adalimumab)
-
Intussusception-
-Intussusception refers to the invagination of a part of the intestine onto itself
-Intussusception is the most common abdominal emergency in early childhood, especially those less than 2 years of age
-The majority of cases intussusception in children are idiopathic
-Intussusception occurs most often near the ileocecal junction.
-The lead point is a lesion or variation in the intestine that is trapped by peristalsis and dragged into the distal segment of the intestine
-Meckel's diverticulum, polyp, tumor, hematoma, or vascular malformation can act as the lead point
-Patients typically develop intermittent crampy, severe progressive abdominal pain, accompanied by inconsolable crying and drawing the legs towards the abdomen.
-Vomiting may follow episodes of abdominal pain
-Between the episodes the child may be pain free
-70 percent of the stools will contain gross blood or occult blood, may be a mixture of blood and mucus (currant jelly)
-Barium enema can be diagnostic and therapeutic
-Surgical resection may be needed if this fails
-Ultrasound or CT scan of Abdomen and Pelvis can diagnose intussusception also
-
Irritable Bowel Syndrome-
-Irritable Bowel Syndrome (IBS) is a GI syndrome defined by chronic abdominal pain and altered bowel habits in the absence of any organic cause
-It is the most common diagnosed GI condition
-IBS is more common in women than men
-Most common presenting symptoms of IBS are chronic abdominal pain, and altered bowel habits
-The chronic abdominal pain is a variable intensity and cramping with periodic exacerbations
-Emotional stress, eating, may exacerbate the pain while defecation usually provides relief
-Things that should increase the suspicion for organic disease causing symptoms include: anorexia, weight loss, rectal bleeding, nocturnal pain, laboratory abnormalities, and malnutrition
-Patients may have diarrhea or constipation both
-The predominate symptom should be treated
-IBS is a diagnosis of exclusion. Patients need to have endoscopy, lab evaluation, or imaging to help rule out organic cause
-
Ischemic Bowel Disease-
-Ischemic bowel disease is caused by a reduction of intestinal blood flow secondary to occlusion, vasospasm, and/or hypoperfusion
-Common sequelae of ischemic bowel include sepsis, bowel infarction, and death
-Acute ischemic bowel refers to sudden onset of intestinal hypoperfusion, which is due to occlusive or non occlusive arterial or venous flow
-Chronic ischemic bowel (intestinal angina) refers to episodic or constant intestinal hypoperfusion which develops with patients with atherosclerotic disease and is strongly associated with eating meals
-Clinical presentation is having a rapid onset of periumbilical pain, which is often out of proportion to physical findings. Nausea and vomiting are usually present
-Risk factors for ischemic bowel include: atrial fibrillation, CHF, peripheral vascular disease, or hypercoagulable state
-Diagnosis is made either with a dynamic CT scan or mesenteric angiography
-Labs usually reveal leukocytosis and metabolic acidosis
-Initial management should include hemodynamic monitoring and support, correction metabolic acidosis, broad spectrum antibiotics, and NG tube for gastric decompression
-Systemic anticoagulation should be administered
-Surgical laparotomy and embolectomy is the traditional treatment for arterial occlusion
-
Lactose Intolerance-
-Clinical symptoms of lactose intolerance include diarrhea, abdominal pain, and flatulence after eating milk or milk containing products
-These symptoms are attributed to low lactase levels which may be due to mucosal injury or much more commonly reduced genetic expression of an enzyme
-Lactose digestion is the rate limited step in the overall process of its absorption.
-Defects in the digestion result in severe diarrhea after intake
-Lactose not absorbed by the small intestine is passed to the colon. In the colon is it is salvaged by converting them to short chained fatty acids
-Major primary causes of lactose malabsorption include: racial or ethnic, developmental, congenital lactase deficiency
-Major secondary causes of lactose malabsorption include: bacterial overgrowth, infectious enteritis, giardiasis, mucosal injury (celiac disease, IBD, or drug/radiation induced enteritis
-Diagnosis of lactose malabsorption is made by a lactose absorption test or lactose breath hydrogen test
-Treatment of lactose intolerance includes: decreased dietary intake of lactose, substitution of nutrient sources to maintain energy and protein intake, administer enzyme substitute, and maintenance of calcium and vitamin D intake
-
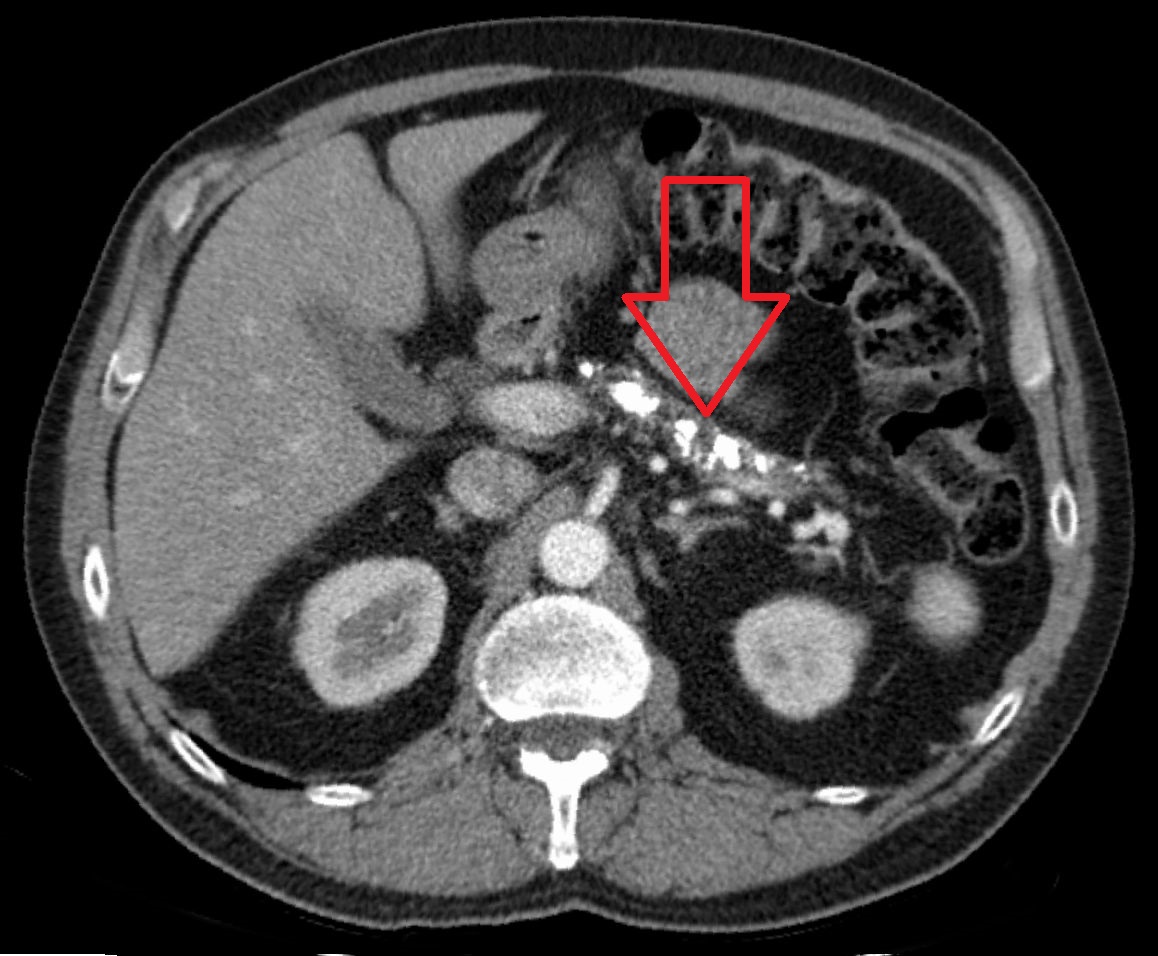
Neoplasms-
-Small intestine tumors are difficult to diagnose because of their rarity and the nonspecific symptoms that they cause
-There are benign (adenoma, leiomyoma, and lipoma) and malignant (adenocarcinoma, carcinoid, lymphoma, and sarcomas)tumors of the small intestine
-Adenocarcinomas are usually between 25-40 percent of small bowel cancers
-Adenocarcinomas can have predisposing factors such as Crohn's Disease and those who have had colorectal cancer
-Carcinoid tumors are well differentiated neuroendocrine tumors that have an indolent disease course. Symptoms generally come from mass effects from the primary or metastatic tumors from production of bioactive amines
-Lymphoma may arise as a primary small intestine neoplasm as a component of systemic disease with GI involvement. Must have no peripheral or mediastinal lymphadenopathy, a normal WBC and differential, tumor involvement must be predominately in the GI tract, and no evidence of spleen or hepatic involvement
-Risk factors for Lymphoma include Autoimmune disease, AIDS, Long Term Immunosuppressive Therapy, Crohn's Disease, Radiation Therapy, or Nodular Lymphoid Hyperplasia
-Sarcomas are malignant mesenchymal tumors that represent about 10 percent of small intestine tumors
-Most common intestinal sarcoma is called a gastrointestinal stromal tumor (GIST)
-Adenomas such as villous and tubular adenomas are benign but have malignant potential
-A Brunner's Gland Adenoma is a rare neoplasm caused by hyperplasia of exocrine glands
-Leiomyomas are single, firm, gray or white well defined masses that arise in the submucosal layer of the wall of the intestine. They are rare benign lesions
-Lipomas are the second most common benign tumor in the small intestine. They occur mostly in the ileum and duodenum
-The vast majority of colorectal cancers are adenocarcinomas.
-Appendix cancer is rare
-Other tumors of the large bowel include Kaposi Sarcoma, lymphomas, and carcinoid tumors
-Tumors are staged in the TMN system
-Ultimate goal eventually is surgical resection
-The tumor marker CEA (Carcinoembryonic Antigen) should be routinely measured preoperatively in patients undergoing potentially curative resections for colorectal cancer
-
Obstruction-
-bowel obstruction occurs when the normal flow of intestinal contents are disrupted
-obstruction can be functional due to intestinal physiology or due to a mechanical obstruction
-Severe small bowel obstruction leads to bowel dilation and retention of fluid within the lumen to obstruction, while the distal obstruction, as lumina contents pass the bowel compresses
-If bowel dilation is excessive, strangulation occurs leading to necrosis or perforation
-Most common causes of small bowel obstruction are post op adhesions and hernias
-SBO can be due to tumor, stricture, intramural hematoma, gallstones, foreign bodies, and intussusception
-Risk factors for SBO include: prior abdominal or pelvic surgery, abdominal wall or groin hernia, intestinal inflammation, neoplasm, prior radiation, or history of FB ingestion
-Clinical symptoms of SBO include abdominal pain, nausea, vomiting, and abdominal dissension
-Will have hypoactive bowel sounds and diffusely tender distended abdomen
-3 view abdomen or CT scan of Abdomen and Pelvis can help confirm the diagnosis
-Treatment is IV hydration, NPO, NG decompression, analgesics, and antiemetics
-Patient may need surgical intervention if it does not resolve with medical therapy
-Large bowel obstruction has similar presentation and treatment but its main causes is neoplasm
-
Polyps-
-Non neoplastic polyps can be grouped into several categories: hyperplastic, mucosal, inflammatory pseudopolyps, and submucosal (some which may be neoplastic-lipomatous and leiomyoma)
-Hyperplastic polyps appear to advance to more advanced lesions and cancer
-Inflammatory pseudopolyps occur with inflammatory bowel disease.
-Mucosal polyps are small and clinical insignificant
-Submucosal polyps include lymphoid aggregates, lipomas, leiomyomas, pneumatosis cystoid intestinalis, hemangiomas, fibromas, carcinoids, and metastatic lesions
-Hamartomas polyps are polyps that are made of tissue elements normally found at the site. Most of the time non neoplastic but some can develop dysplasia and lead to colorectal cancer
-common neoplastic colonic polyps include serrated polyps and adenomatous polyps
-Most studies suggest the development of cancer from adenomatous polyps is 7-10 years
-Treatment of these polyps is endoscopic removal
-Surveillance is recommended every 10 years after negative colonoscopy or 3-5 years after polyp removed
-Recommended colorectal screening is starting at age 50 or 10 years younger than a first degree relative with colorectal cancer
-Toxic Megacolon-
-Toxic Megacolon is a potentially lethal complication of inflammatory bowel disease or infectious colitis
-It is characterized by total or segmental non obstructive colonic dilation plus system toxicity
-Colonic dilation is also observed in patients with congenital megacolon (Hirschsprung's Disease), idiopathic or acquired megacolon occurring with chronic constipation, and intestinal pseudo obstruction, a manifestation of diffuse GI dysmotility of various causes
-Etiology of toxic megacolon is mostly IBD, but also can occur with infectious colitis, volvulus, diverticulitis, ischemic colitis, and obstructive colon cancer
-One possible pathogenic mechanism is that mucosal inflammation leads to release of inflammatory mediators and bacterial products, increased nitrous oxide synthase, gene ratio of excessive nitric oxide and colonic dilation
-Signs and symptoms include: severe blood diarrhea, malaise, and abdominal pain and dissension
-The transverse colon is dilated greater than 6 cm and up to 15 cm on supine films
-CT scan of Abdomen and Pelvis is recommended
-The main goal of treatment is to reduce the severity of the colitis and restore normal colon motility and decrease the likelihood of perforation. Surgical consult should be obtained on admission up to 50 percent of patients may fail medical therapy and require surgical treatment